Received: Mon 31, Jul 2023
Accepted: Tue 29, Aug 2023
Abstract
Purpose: Accident or abuse play a role in the etiology of genital, anal and perineal traumas in children. It was aimed to evaluate the genital injury scores and treatment modalities of patients injured as a result of accidents. Methods: After the approval of the local ethics committee, the files of the patients who were treated for genital, anal and perineal trauma in a tertiar center between November 2011 and December 2021 were reviewed retrospectively. An evaluation was made by revealing the gender, age, mechanism of trauma, physical examination findings and treatment modalities of the patients. Results: In this period 59 patients including 30 male and 29 female were treated with mean age of 7.5 year. Genital injury score was determined in trauma caused by running, walking or falling on an object, falling off a bicycle, fighting and non-vehicle traffic accident. Penile hematoma, abrasion, tissue defect, scrotal edema-hematoma-pain, laceration, testicular pain, perineal-perianal laceration, labium majus-minus laceration, abrasion, tissue defect, hymen laceration, laceration in anal sphincter and rectal mucosa were observed. In addition to medical treatment, primary repair, perineoplasty, colostomy, anoplasty, hymenoplasty, sphincteroplasty and debridement were performed. Recovery was uncomplicated. Conclusion: The most common cause of trauma in children is falls, and patients with low genital injury scores on physical examination require medical treatment and/or primary repair with local anesthesia, while those with high levels require examination and surgical treatment under general anesthesia.
Keywords
Child, genital-anal-perineal trauma, genital injury score, accident
1. Introduction
Genital trauma and perineal injury are rare in children. Injuries include falling off a bicycle, hitting playgrounds or swimming pools, hitting furniture corners or shower edges, falling on toys, falling from trees, traffic accidents, burns, penetrating injuries, and sexual abuse. Anal injuries can occur in a spectrum ranging from minimal laceration involving only the anus to rectal avulsion [1]. It is caused by traffic accidents, falls and sexual abuse, respectively [2]. Treatment varies according to the localization and depth of the injury [3]. Trauma to the genital area has consequences that affect aesthetic, functional, psychological and quality of life [4]. In our study, approach and treatment options for genital, anal and perineal injuries in the pediatric population were evaluated.
2. Materials and Methods
After the approval of Selcuk University Faculty of Medicine Local Ethics Committee (2021/527), the files of patients treated for genital, anal and perineal trauma in the pediatric surgery clinic between November 2011 and December 2021 were reviewed retrospectively. The gender, age, mechanism of trauma, physical examination findings and treatment modalities of the patients were determined and evaluated. Patients with cranial, thoracic and abdominal organ injuries were not included in the study. Onen’s classification was used to classify the genital, anal, and perineal injuries (Table 1).
TABLE 1: Onen’s classification for genital
injuries in children.
|
GIS |
Extend of injury |
|
|
|
|
I |
Isolated genital laceration
below hymen or limited to penile/scrotal skin
|
|
II |
Isolated genital laceration
including hymen or tunica dartos of scrotum/Bucks fascia of penis
|
|
III |
Isolated genital laceration
including vagina or testis/penile cavernous or distal urethra
|
|
IV |
GIS II or III injury plus
partial tear of anorectum
|
|
V |
GIS III injury plus complete
tear of anorectum |
|
|
|
|
|
GIS genital injury score |
3. Results
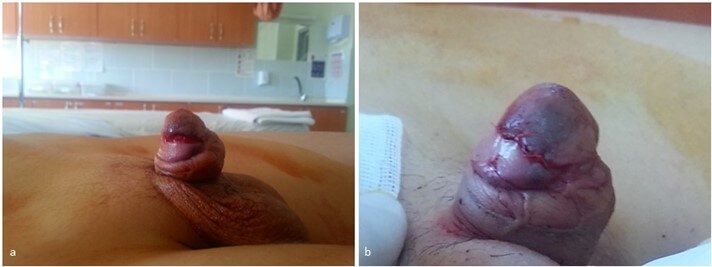
Between the specified dates, a total of 59 patients, 30 boys and 29 girls, were treated in our clinic for genital, anal and perineal trauma. The mean age of the patients was 7.5 years. Etiology was found to be running, walking or falling on an object in 38 patients, falling off a bicycle in 16 patients, kicking in 4 patients, and a traffic accident outside of a vehicle in 1 patient (Table 2A). Penile hematoma-abrasion-tissue defect (Figure 1), scrotal edema-hematoma-pain-laceration, testicular pain, perineal-perianal laceration were found in boys, and labium majus-minus abrasion-laceration (Figure 2), superior urethra laceration to the clitoris, hymen laceration (Figure 3) and perineal-perianal laceration were found in girls. Genital injury score was found as 1 in 46 patients, 3 in 7 patients, 3 in 4 patients, 4 in 3 patients and 5 in 2 patients. In boys, medical treatment (antibiotic ointment, antibiotherapy, analgesia) was performed in 20 patients, primary repair with local anesthesia in 5 patients, primary repair under general anesthesia in 2 patients, debridement in 1 patient, perineoplasty- sphinkeroplasty-colostomy in 1 patient, and anoplasty-colostomy in 1 patient. In girls, medical treatment (antibiotic ointment, antibiotherapy, analgesia) was performed in 19 patients, primary repair under local anesthesia in 2 patients, primary repair under general anesthesia in 4 patients, perineoplasty in 2 patients, perineoplasty-hymenoplasty in 1 patient, and perineoplasty-sphincteroplasty in 1 patient (Table 2B). After the anogenital injuries of two patients who underwent colostomy were checked under general anesthesia, their colostomies were closed. No anal incontinence was observed in the follow-up patients who underwent sphincteroplasty.Descriptive analyses were used for statistics.
TABLE 2A: Patient characteristics.
|
|
|
|
|
|
n
(%) |
||
|
Age (year old) |
|
|
|
median |
7.5(3-17) |
||
|
Gender |
|
|
|||||
|
male |
30(50.2%) |
|
|||||
|
female |
29(49.8%) |
|
|||||
|
Etiology |
|
|
|
|
|
||
|
falling during running,
walking, or on an object |
|
|
|
|
38(64.3%) |
||
|
falling from bicycle |
|
|
|
|
16(27.2%) |
||
|
kicking in a fight |
|
|
|
|
4
(6.8%) |
||
|
traffic accident |
|
|
|
|
1
(1.7%) |
||
TABLE 2B: Genital injury score and
treatment.
|
GIS |
Treatment (n) |
|||||||
|
|
medical |
primary suture |
perineo plasty |
colostomy |
ano plasty |
hymeno plasty |
sphincteroplasty |
debridement |
|
I |
37 |
3 |
3 |
|
|
|
|
|
|
II |
1 |
6 |
|
|
|
|
|
|
|
III |
1 |
3 |
|
|
|
|
|
|
|
IV |
|
1 |
1 |
|
|
1 |
|
2 |
|
V |
|
|
1 |
2 |
2 |
|
2 |
|
GIS: genital injury score; n: number of
patients.


4. Discussion
Accidental genital trauma and perineal injury are rare in the pediatric population. Injuries include falling off a bicycle, hitting playgrounds or swimming pools, hitting furniture corners or shower edges, falling on toys, traffic accidents, burns, penetrating injuries, and sexual abuse. Erythema, ecchymosis, hematoma, abrasion, hymen laceration and vaginal laceration may be seen in genital area injuries, as well as normal physical examination findings [5].
It should be kept in mind that most of the sexually abused patients may have normal physical examination findings. In a study evaluating the findings of sexual abuse in children and adolescents, diagnostic findings of trauma or sexual contact were detected in less than 5% of the patients as a result of 3569 examinations [6]. The presence or suspicion of sexual abuse was not observed in the cases treated in our clinic.
In a study evaluating girls under the age of 15 with accidental genital trauma, it was stated that the time of hospital admission, type of injury, and wound size affected surgical treatment, and 24% of 159 patients in the study were treated surgically [7]. Primary repair was performed under local anesthesia in the adolescent and cooperative patient group. In our study, 27.6% of the female patients were treated, and 6.7% were treated locally, while 16.7% of the male patients were treated after general anesthesia and 13.4% were treated after local anesthesia. We think that the presence of additional organ injury, wound size and patient age are factors in this.
In a study evaluating 75 patients treated over a 20-year period, fall from height, traffic accident and sexual abuse were reported as etiological factors, and patients underwent vaginoplasty, anoplasty, perineoplasty, sphincteroplasty, hymenoplasty, primary repair, secondary healing, and colostomy [8]. Considering the etiological factors, sexual abuse was not found in our patient group. Surgical applications are similar except for vaginoplasty. Fall as the cause of injury was also seen as the most common factor in our study.
In a study examining the characteristics of accidental genital trauma in young girls and indications for surgical treatment, 137 patients were evaluated. Impact on the thigh-groin region was the most common cause, and labial injury was the most common, and 12.1% of the patients were operated [9]. The mechanism of trauma was similar to our patient group, and 12 of 29 female patients included in our study had labial injury. In addition to medical treatment, primary repair was most frequently performed.
In a study that included 359 patients in which the characteristics of accidental genital trauma in girls were evaluated, it was stated that injuries of 3 cm and above and injuries to the hymen, vagina, urethra and anus should be treated surgically [10]. In our study, surgical treatment was applied to patients with similar findings.
In a study examining 41 patients in whom sexual injury and impalement injury often play a role in the etiology, the patients were divided into three groups as perineal and genitourinary, perineal and anorectal, and perineal genitourinary and anorectal injuries [11]. We have classified it differently according to the genital injury score, which is more comprehensive. However, primary repair was performed in all patients in the treatment, and in our study, there were patients who were treated with medical treatment according to the severity of the injury. We can state that medical treatment will be sufficient for patients with genital injury score of 1 in the first examination in the emergency department.
The operation technique was described based on the rules of posterior sagittal anoplasty (PSARP) technique after colostomy in three patients with full-thickness vaginal separation and anal sphincter rupture as a result of sexual assault. After placing a lonestar retractor and suspending sutures, the anterior wall of the rectum and the vagina were separated and repaired [12]. Although traumas related to sexual abuse were excluded from the study, repair was performed with the anterior approach after colostomy in 2 patients with a GIS score of 5, and with the anterior approach in 3 patients with a GIS score of 4. Postoperative incontinence was not observed in our patients and recovery was uneventful.
Successful results were obtained by performing repairs similar to the PSARP technique in 2 patients with a GIS score of 4 as a result of falling, in which the primary repair was unsuccessful [13]. Although the described technique is used in very few cases in the literature, we think that it can be an alternative in secondary cases.
In a study examining pediatric vulva-vaginal lacerations, straddle injuries were identified as the most common cause. Superficial injuries with an average size of 1.1 cm were detected in 60.7% of the cases. 34.8% of the patients were sedated in the emergency room and 4.8% were operated in the operating room [14]. In our study, male patients were also evaluated, and 19 (65%) of the female patients and 20 (66%) of the male patients were discharged with medical treatment. In addition, those with the appropriate age and injury pattern were treated with local anesthesia, while the others were treated in the operating room.
In a study evaluating genital trauma characteristics in adult male patients, it was stated that infectious causes such as fournier's gangrene, penile and scrotal skin injuries, burns, testicular and spermatic cord injuries, penile fracture and amputation were the causes [4]. Penile and scrotal skin injuries from the causes described in the adult patient group were present in our patients. Penile fracture is very rare in children, and rupture of the corpus cavernos was detected due to the development of penile pain, hematoma and ecchymosis in a 7-year-old child who hit the stair railing as a result of falling [15]. Penile fracture was not detected in our patients who were treated with similar complaints.
Degloving injuries of male perineum are very rare. A 10-year-old boy lost his penile shaft skin as a result of his shorts getting stuck in the fan belt of the milling machine. He recovered uneventfully after treatment with a graft taken from the forearm [16]. Although tissue defects and lacerations were observed in our study, our patients did not need grafts.
Anogenital traumas in children generally occur as a result of falling on the thigh-groin area. Superficial injuries should be treated with medical treatment, young people, cases where the wound cannot be visualized well, those with uncontrollable bleeding and complicated injuries should be examined under general anesthesia and treated appropriately according to the injured area and wound size.
5. Conclusion
The most common cause of trauma in children is falls, and patients with low genital injury scores on physical examination require medical treatment and/or primary repair with local anesthesia, while those with high levels require examination and surgical treatment under general anesthesia. Recovery is usually uncomplicated and the prognosis is good.
Author Contributions
All authors have made substantial contributions to all of the following: i) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, ii) drafting the article or revising it critically for important intellectual content, iii) final approval of the version to be submitted.
Compliance with Ethical Standards
Selcuk University Faculty of Medicine Local Ethics Committee (2021/527).
Conflicts of Interest
None.
REFERENCES
[1] Inbal Samuk, Zvi Steiner, Elad
Feigin, et al. “Anorectal injuries in children: a 20-year experience in two
centers.” Pediatr Surg Int, vol. 31, no. 9, pp. 815-819, 2015. View at: Publisher Site | PubMed
[2] M G Scheidler, B L Schultz, L Schall,
et al. “Mechanisms of blunt perineal injury in female pediatric patients.” J
Pediatr Surg, vol. 35, no. 9, pp. 1317-1319, 2000. View at: Publisher Site | PubMed
[3] Abdurrahman Onen, Hayrettin Oztürk,
Murat Yayla, et al. “Genital trauma in children: classification and
management.” Urology, vol. 65, no. 5, pp. 986-990, 2005. View at: Publisher Site | PubMed
[4] James Furr, Daniel Culkin “Injury to
the male external genitalia: a comprehensive review.” Int Urol Nephrol,
vol. 49, no. 4, pp. 553-561, 2017. View at: Publisher
Site | PubMed
[5] Laura J Benjamins “Genital trauma in
pediatric and adolescent females.” J Pediatr Adolesc Gynecol, vol. 22,
no. 2, pp. 129-133, 2009. View
at: Publisher
Site | PubMed
[6] Tanya D Smith, Sudha R Raman, Sheri
Madigan, et al “Anogenital Findings in 3569 Pediatric Examinations for Sexual
Abuse/Assault.” J Pediatr Adolesc Gynecol, vol. 31, no. 2, pp. 79-83,
2018. View at: Publisher
Site | PubMed
[7] Kidong Kim, Jae Hong No, Yong-Beom
Kim, et al. “Patterns of accidental genital trauma and factors associated with
surgical management in girls visiting the emergency department of a referral
center.” J Pediatr Adolesc Gynecol, vol. 27, no. 3, pp. 133-137, 2014. View at: Publisher Site | PubMed
[8] U Bakal, M Sarac, T Tartar, et al.
“Twenty years of experience with perineal injury in children.” Eur J Trauma
Emerg Surg, vol. 42, no. 5, pp. 599-603, 2016. View at: Publisher Site | PubMed
[9] Corey W Iqbal, Nezar Y Jrebi, Martin
D Zielinski, et al. “Patterns of accidental genital trauma in young girls and
indications for operative management.” J Pediatr Surg, vol. 45, no. 5,
pp. 930-933, 2010. View
at: Publisher
Site | PubMed
[10]
Tazim Dowlut-McElroy, Jeanette Higgins, Karen B Williams, et al.
“Patterns of Treatment of Accidental Genital Trauma in Girls.” J Pediatr
Adolesc Gynecol, vol. 31, no. 1, pp. 19-22, 2018. View at: Publisher Site | PubMed
[11] Darshan
A Manjunath, Veerabhadra Radhakrishna, Deepti Vepakomma “The Management of
Perineal Trauma in Children.” J Indian Assoc Pediatr Surg, vol. 27, no.
1, pp. 65-70, 2022. View
at: Publisher
Site | PubMed
[12] Giulia
Brisighelli, Marc A Levitt, Richard J Wood, et al. “A Surgical Technique to
Repair Perineal Body Disruption Secondary to Sexual Assault.” European J
Pediatr Surg Rep, vol. 8, no. 1, pp. e27-e31, 2020. View at: Publisher Site | PubMed
[13] Adewale
Olaotan Oyinloye, Samuel Wabada, Christopher Uruku Rikin, et al. “Surgical
management of traumatic perineal injury in female children: A report of two
cases.” Int J Surg Case Rep, vol. 103, pp. 107874, 2023. View at: Publisher Site | PubMed
[14] Nathaniel
Ladaga, Meredith Busman, Lindsey Ouellette, et al. “Pediatric vulvo-vaginal
lacerations in a community-based population.” Am J Emerg Med, vol. 55,
pp. 194-195, 2022. View
at: Publisher
Site | PubMed
[15] Blake C Gruenberg, David Mortel, Amanda Bogie “Rupture of the Corpus Cavernosum in a Pediatric Patient.” Pediatr Emerg Care, vol. 37, no. 2, pp. e73-e74, 2021. View at: Publisher Site | PubMed
[16] O O Onumaegbu, O C Okechukwu “Isolated penile degloving from milling machine injury in a child.” Ann Med Health Sci Res, vol. 5, no. 2, pp. 139-141, 2015. View at: Publisher Site | PubMed